| Want to send this page or a link to a friend? Click on mail at the top of this window. |
| Posted February 18, 2007 |
| Unequal Treatment | ||
| _____________________________________________ | ||
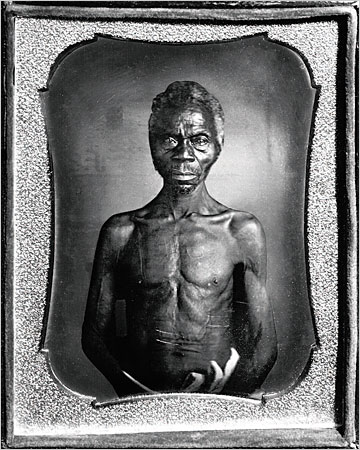
| Harriet Washington investigates the exploitation of African-Americans in medical research. | ||
 |
||
|
| _____________________________________________ |
| MEDICAL APARTHEID | |
| The Dark History of Medical Experimentation | |
| on Black Americans. From Colonial Times | |
| to the Present | |
| By Harriet A. Washington. | |
| Illustrated, 501 pp. Doublrday. $27.95 | |
| By EZEKIEL EMANUEL |
IN April 1721, sailors arriving from Barbados set off a smallpox epidemic that raged in Boston for a year. Cotton Mather, the powerful Puritan minister, advocated using pus from a smallpox scab to infect another person, producing a mild case and long-term immunity to the “speckled monster.” Mather first learned about inoculation from an African slave and from reports of the practice in Turkey. For years, he had repeatedly failed to persuade any physician to try it. But on June 26, 1721, Zabdiel Boylston, a physician, administered pus to his 6-year-old son and two of his slaves, an adult and child. All three experienced mild cases and quickly recovered. By the time the epidemic subsided, Boylston had inoculated 244 people, six of whom died — a death rate of 2.4 percent, compared with 14 percent for the nearly 6,000 Bostonians who acquired smallpox naturally.
| The history of medical abuse of blacks, Washington charges, goes far beyond the Tuskegee study. |
As Boylston’s use of slaves highlights, African-Americans have participated in biomedical research from the outset. In “Medical Apartheid,” Harriet Washington charges that they have also too often been abused and exploited by a racist medical establishment. This history, she argues, goes far beyond the infamous Tuskegee syphilis study, in which African-American sharecroppers, under the sponsorship of the United States Public Health Service, were for 40 years subjected to various procedures and prevented from getting penicillin treatment — despite the fact that determining the course of the disease, the putative goal of the study, had already been accomplished. “Researchers who exploit African-Americans,” Washington writes, “were the norm for much of our nation’s history, when black patients were commonly regarded as fit subjects for nonconsensual, nontherapeutic research.”
Washington, a journalist and former ethics fellow at Harvard Medical School, tells some harrowing stories, and claims that throughout the 19th century, medical schools disproportionately used blacks in live surgical demonstrations. In more recent times, she writes, they have been disproportionately enrolled in risky, nonbeneficial research in gynecology, oncology, surgery, pediatrics, infectious disease and genetics. While the worst excesses are a thing of the past, blacks are still “at greater risks than whites of being conscripted into ... research without giving their consent.”
There have been superb studies of individual cases of exploitation, particularly James H. Jones’s masterful 1981 history of Tuskegee, “Bad Blood.” Yet we lack a comprehensive history of the role of African-Americans in research. Unfortunately, “Medical Apartheid” is not that book. Washington’s polemic fails in two ways. First, it fails to place the experience of African-Americans in a broader social, historical, scientific and ethical context, comparing it with that of research participants more generally. Second, the book is so riddled with exaggerations, distortions, contradictions, errors and confusions as to be untrustworthy.
The history of medical research in America has seen tragedies and triumphs, instances in which exploitation occurred and others in which measures were taken to minimize it. For example, in his yellow fever research of 1900-1, Walter Reed delineated many safeguards, including auto-experimentation (members of his Yellow Fever Board would themselves be research subjects), a signed contract with participants (forerunner of today’s informed-consent documents) and a prohibition against doing research on children until after it had been successfully completed on adults. Amazingly, the only person to die in this very high-risk research was Jesse Lazear, a white medical school graduate and a member of the board. Since Tuskegee and other scandals, further safeguards have been enacted, including the establishment of independent review boards charged with ensuring that research is scientifically valid, that participants give informed consent and that the benefits outweigh the risks. While not perfect, these safeguards have minimized the risk of abuse.
Still the question remains: Why have some researchers exploited certain groups? For Washington, the answer comes down to one thing: skin color. “The racial homogeneity of American medical researchers,” she writes, “lies at the very heart of the problem.”
Doubtless, many American researchers in the past were — and some current ones may still be — racist. But this explanation is simplistic. Risky research — whether beneficial or not — has often relied on various vulnerable populations, including the elderly, soldiers, prisoners, the mentally disabled and orphans of all races and creeds. Yes, African-Americans have been exploited, but they have not been singled out exclusively or even predominantly. In the so-called Jewish Chronic Disease Hospital case of 1963, for instance, prominent researchers injected live cancer cells into nursing home residents, some of whom were Holocaust survivors, to determine whether the immune systems of sick individuals could identify and eliminate foreign cancer tissue as those of healthy people do — a classic case of “nonconsensual, nontherapeutic experimentation.” Today, probably the research with the highest risk and lowest benefit to participants is Phase I cancer research, which tests experimental cancer drugs to determine the highest tolerable dose for subsequent studies. More than 85 percent of participants of such research are white and two-thirds have college educations.
A more plausible explanation can be traced to the fact that, as the medical historian David Rothman has argued, medical research — especially in the decades after World War II — was “unabashedly utilitarian.” The government and pharmaceutical industry invested substantially to develop vaccines, antibiotics and other drugs, and to assess radiation and other toxicities. Enrolling vulnerable people in research was justified as providing a way they could contribute to society. As Walsh McDermott, one of the most prominent academic physicians of the past century, put it at a 1967 colloquium: “We have seen large social payoffs from certain experiments in humans. ... We could no longer maintain, in strict honesty, that in the study of disease the interests of the individual are invariably paramount.”
This was not just the view of scientists but also of much of the public; many guardians of the institutionalized children in the safety test of Jonas Salk’s polio vaccine, for example, said they felt honored to have their children be part of the risky research. Thankfully, few researchers (or parents) would express such views today. But they reveal the mind-set of those who could accept, even if they did not themselves commit, exploitative research.
Despite its many footnotes and its claim to be meticulously researched in long-ignored archives, “Medical Apartheid” is suffused with undocumented assertions and factual errors. Consider this typical claim: “Of the first 251 experimental inoculations of smallpox by Dr. Zabdiel Boylston in predominantly white Brookline, Massachusetts, all but one of the subjects were black.” In fact, according to Boylston’s own 1726 report, he inoculated 244 people, of whom 12 were identified as black, 4 as Native American and 12 as servants and others of unspecified race. The rest, including Boylston’s six children, were white.
Another example, from Washington’s introduction: “Within recent years,” she writes, the Office for Protection From Research Risks has “suspended all research at such revered universities as Alabama, Pennsylvania, Duke, Yale and even Johns Hopkins. Many studies enrolled only or principally African-Americans.” But research at Pennsylvania and Yale has never been suspended by that agency (which is now called the Office for Human Research Protections) or any other federal regulator; at Alabama, only some research was restricted. More importantly, the suspensions at the other institutions had nothing to do with concerns over minority enrollment. At Johns Hopkins, for instance, research was suspended for three days in 2001 following the death of a healthy, white 24-year-old volunteer in an asthma study. At Duke, where research was suspended for five days in 1999, the problems mainly involved record-keeping and other technical aspects of the monitoring of consent.
Throughout the book, Washington blurs the distinction between “experimentation” and routine medical care and public health measures, recounting ordinary events as if they were shockingly unethical research practices. The chapter “The Black Stork,” for example, hardly mentions research at all. Instead, Washington condemns the distribution of contraceptives to young black women by Planned Parenthood and others, whose practices she links to eugenics. Similarly, the chapter on infectious disease opens with the story of an African-American man who was legally detained to ensure he took his tuberculosis medication. Whatever the ethics of this particular case, it concerns quarantine practices, not research. (Patients who follow treatment only erratically contribute to the rise of dangerous drug- resistant strains.) Washington then seems to dismiss directly observed therapy, in which patients must be watched ingesting a complex sequence of medication daily, as yet another of the “inequitable policies” — blacks have a 300 percent greater risk of contracting tuberculosis than whites — that have “shaped the uncomfortably close relationship between African-Americans and infectious disease.”
In a discussion of how “medical sadism” has been exported to Africa, Washington writes that “third world women subjects of thalidomide trials for leprosy and AIDS were not warned of the horrible birth defects the drug can cause.” As with many of Washington’s inflammatory claims, there is no citation. And her implication that third world women bear the brunt of this research is simply wrong. Of the six controlled clinical trials of thalidomide for leprosy (which were actually conducted between 1965 and 1971), those in Israel, Venezuela, Malaysia and the United States enrolled men or postmenopausal women, while trials in India, Mali, Somalia and Spain enrolled only men. Furthermore, one of the largest longitudinal studies of thalidomide for leprosy did not single out third world women at all but was done in the United States, Canada and United States territories.
Washington says that she wrote “Medical Apartheid” in order to help close the “health gap” that afflicts African-Americans — a gap she blames in large part on the untrustworthiness of the medical establishment, which leads many blacks to avoid care. The gap is certainly real: today, blacks die younger than whites, have substantially higher infant mortality rates and receive fewer medical services. Documenting the history of medical research involving black Americans is a necessary and worthy project, but a book as rife with errors and confusions as this one will neither help reduce health disparities nor protect against future exploitation.
Ezekiel Emanuel is an oncologist and chairman of the department of clinical bioethics at the National Institutes of Health. He is co-editor of the forthcoming book “Ethical Issues in International Biomedical Research.”
Copyright 2007 The New York Times Company. Reprinted from The New York Times, Book Review, of Sunday, February 18, 2007.
| Wehaitians.com, the scholarly journal of democracy and human rights |
| More from wehaitians.com |